
IGF-1 LR3
🔍 Description:
IGF-1 LR3 is a potent analog of insulin-like growth factor-1 (IGF-1) that has been modified to extend its half-life, allowing for prolonged anabolic effects. It plays a crucial role in muscle growth, recovery, and overall anabolic activity by mimicking the natural effects of IGF-1 with enhanced potency.
💪 Health Benefits:
– Muscle Growth: Significantly enhances lean muscle mass and strength, making it popular among bodybuilders and athletes.
– Recovery: Speeds up recovery from injuries and intense workouts, reducing downtime and improving training outcomes.
– Fat Loss: Supports fat metabolism and improves body composition by increasing muscle-to-fat ratio.
💉 Dosing/Administration:
– Typical Dosage: 50-100 mcg daily, often administered post-workout.
– Administration Method: Subcutaneous injection, typically in muscle areas for localized effects.
– Cycling: Typically used in cycles of 4-6 weeks, followed by breaks to prevent desensitization and maintain effectiveness.
⚠️ Side Effects and Safety:
– Common Side Effects: Potential hypoglycemia, water retention, and risk of promoting the growth of existing tumors.
– Safety Profile: Should be used under medical supervision due to its potent effects, particularly in individuals with a history of cancer or metabolic disorders.
GH secretagogues are some of the most popular peptides around and with it, the popularity of monitoring methods.
Most are already familiar with IGF-1 and why it’s used as surrogate for GH secretions (related to much less daily fluctuations and longer half life).
We don’t usually discuss the details of the “long half life” but now it’s becoming more relevant.
IGF-1 is 70-amino-acid long, weighing 7.6 kDa, it’s made mainly by the liver in response to GH. IGF-1 is a hormone (look up the definition of “hormone”) that is generally anabolic and mediates many of GH’s functions.
Side note: another name for IGF-1 is “somatomedin c”
IGF-1 is just another protein that actually, as a stand-alone, has a SHORT half-life, we’re talking maybe 10 minutes? That’s not much better than GH! But wait.
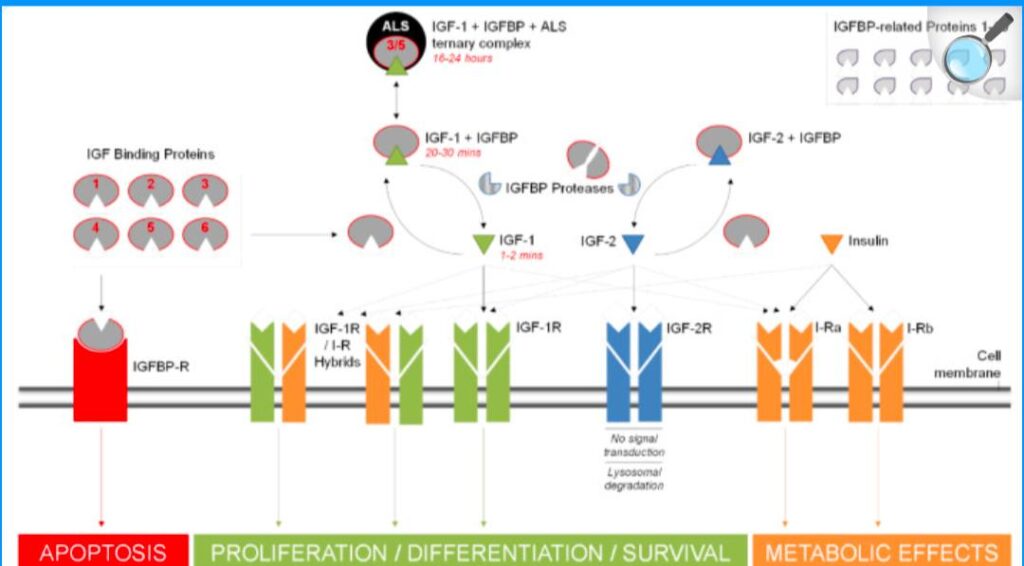
IGF can bind with 2 additional things: IGF-binding proteins (IGFBP) and Acid Labile Subunit (ALS).
When IGF binds to IGFBP3 forming a so-called “binary” complex, its half-life is extended to maybe 30-90 minutes. And when ALS is added to this, forming a 3-prong complex called “ternary”, it becomes even much more stable with a half life averaging 15 hours.
To summarize about half lives:
Free IGF-1 = 10 min
IGF-1 + IGFBP3 = 30 – 90 min
IGF-1 + IGFBP3 + ALS = 15 hours
Free IGF-1 is supposedly biologically active, while the bound forms act as a reservoir for steady supply.
…The commercially available IGF measurements are typically the TOTAL IGF-1. The Free IGF-1 is usually only available in research setting, as it’s very tricky to measure accurately. I’m not a chemist or a laboratory technologist but from my limited understanding, the difficulties arise from:
– instability and short half life of free IGF-1
– interference from the IGFBP(s) on the assay method
– difficult to separate/isolate the serum free IGF-1 from the bound ones and IGFBP(s) in the sample
There has been no universally accepted method for free IGF-1 analysis, let alone a standard reference range. So we’re left with Total IGF-1.
Total IGF-1, imperfect as it is, has been the standard measurement for monitoring, even in clinical medicine with the most experience at this: pediatric endocrinology practice of hGH replacement for true GH Deficiency
.
But even here we have different methods. A big example:
– LabCorp uses IDH-iSYS immunoassay method
– Quest uses LC/MS method
These are the 2 biggest commercial labs in the US. Someone smarter than me in assay technique can double check and correct me if I’m wrong, but my understanding is that while LCMS technique is often considered better than radioimmunoassay, however, the IDH-iSYS immunoassay system has been widely validated and is the current standard for total IGF-1 measurement in the world of medicine & research at the moment.
Each method has their own normal reference ranges (not to mention other less popular measurements methods), which is probably why if you’re trying to find normal IGF level, you’ll get several different answers.
If we are trending our total IGF-1 levels over time, it’s probably best to:
1. Use the same lab/method
2. Use the reference range provided by the lab, because that range is specific to the method used
In clinical trials it seems IGF-1 levels tend to plateau anywhere between 2-4 weeks of continuous use, and falls back to baseline also in about the same 2-4 weeks time after stopping
. It’s understandable that some aren’t satisfied with Total IGF-1 alone.
IGFBP3 measurement (and using total IGF-1/IGFBP3 ratio) is an attempt to deduce the “free IGF-1” level indirectly. Noble effort but imperfect. Best case scenario it’s unnecessary, worst case it’s potentially misleading.
Reasons:
1. While IGFBP3 takes the lion’s share of IGF-1 binding, there are at least 6 IGFBP(s) running around
2. Factors affecting IGFBP3 levels (other than GH) are incompletely understood
3. IGFBP3 has other functions besides carrying IGF-1 and we don’t know how these other functions affect its level & relationship with IGF-1
4. IGFBP3 measurement method is still being perfected
5. In the early phase of GH increase (whether by exogenous hGH, or by GH secretagogues use), liver productions of both IGF-1 and IGFBP3 rise almost equally, but at the latter phase, as GH level increases more, it seems that IGF-1 production outpaces IGFBP3. Translation: more biologically active free IGF-1 available.
6. Hence for now, total IGF-1 level should be a good indicator of therapy efficacy. In fact this is currently the accepted standard of therapy monitoring for both hGH replacement in pediatrics world, and Tesamorelin use in HIV/HAART patients
. As a side note, there was a cohort study by Mayo Clinic trying to follow Total IGF-1, IGFBP3, and IGF/IGFBP3 ratio in the elderly population (50 – 95 y/o) measured up to 5 years (average 2.3 yrs follow up). They used Siemens Immulite 2000 immunoassay, and I find this study very interesting because:
1. Total IGF-1 has NEGATIVE correlation with age (of course!)
2. IGFBP3 also has NEGATIVE correlation with age (makes sense)
3. But, IGF/IGFBP3 ratio has a POSITIVE correlation with age. Meaning, your IGFBP3 goes lower faster than your total IGF-1! What’s the implication? Could it be that actually our serum free IGF-1 remains pretty stable over our lifetime? That is the question!
Of course science keeps progressing and at some point once we understand the whole physiological dynamics of IGFBP3 and/or come up with a reliable standardized method of IGFBP3 measurement, practice pattern will change.
For now I’m just not sure that measuring IGFBP3 adds any significant value for most people. We’re not sure if it’s accurate, we’re not sure what the standard reference should be, we’re not completely sure of the factors affecting it, and most importantly we aren’t sure what adjustments to do with the results.
We can certainly measure it for academic curiosity, but just be careful with what you do with that information.
Maybe someday we’ll be able to directly measure free IGF-1 level with precision and we can do away with all this guesswork. That’s what we do with thyroid hormone therapy monitoring these days, allowing us precise adjustments.
We can only hope
. Below are articles for reading:
Challenges of insulin-like growth factor-1 testing
https://www.tandfonline.com/doi/full/10.1080/10408363.2024.2306804#abstract
Reference Values for IGF-I Serum Concentrations: Comparison of Six Immunoassays
https://pmc.ncbi.nlm.nih.gov/articles/PMC5054194/
Antibody-free LC-MS/MS method for the quantification of intact insulin-like growth factors 1 and 2 in human plasma, compared to IDH-iSYS
https://pmc.ncbi.nlm.nih.gov/articles/PMC7943504/
Trajectories of plasma IGF-1, IGFBP-3, and their ratio in the Mayo Clinic Study of Aging
https://pmc.ncbi.nlm.nih.gov/articles/PMC5911407/
Evaluation of IGF1/IGFBP3 Molar Ratio as an Effective Tool for Assessing the Safety of Growth Hormone Therapy in Small-for-gestational-age, Growth Hormone-Deficient and Prader-Willi Children
https://pmc.ncbi.nlm.nih.gov/articles/PMC6745465/#:~:text=The%20IGF1/IGFBP3%20molar%20ratio%20was%20calculated%20according,x%200.13]%20/%20[IGFBP%2D3%20(ng/mL)%20x%200.035].&text=The%20three%20study%20groups%20were%20heterogeneous%2C%20differing,and%20IGF/IGFBP3%20molar%20ratio%20increases%20with%20age.
Presentation of IGF-1/IGFBP-3 molar ratio as an effective monitoring index during treatment of growth hormone deficient patients
https://abstracts.eurospe.org/hrp/0094/hrp0094p2-259
LabCorp IGF-1 IDH-iSYS
https://www.labcorp.com/tests/010363/insulin-like-growth-factor-1-igf-1
Quest IGF-1 LC/MS
https://testdirectory.questdiagnostics.com/test/test-detail/16293/igf-1-lc-ms?cc=MASTER